

Abstract
Background: Personalizing treatment of hemophilia A includes tailoring the product and regimen to patient characteristics and lifestyle. Factor VIII (FVIII) pharmacokinetic (PK) parameters such as peaks and troughs, area under the curve, and time spent below a certain FVIII level may be important factors in determining risk for hemarthroses or other bleeds, particularly during periods of high activity when patients are at risk of traumatic bleeding. It is important to identify which patients may be most appropriately treated with different products/regimens. Given a lack of real-world outcomes data, modeling offers a way to estimate bleeding risk with various regimens for different physical activity profiles.
Aim: This outcomes research model estimated the relative bleeding risk for different patient physical activity profiles associated with various prophylaxis regimens using standard half-life recombinant FVIII (SHL-rFVIII) and extended half-life rFVIII (EHL-rFVIII), as well as with scenarios based on a theoretical baseline FVIII activity level with minimal variance.
Methods: A 1-compartment PK model (Collins, et al. Haemophilia 2011) was used to predict FVIII activity associated with different treatment regimens. For SHL-rFVIII and EHL-rFVIII, half-life (10.4 and 14.3 hours, respectively) and incremental recovery (2.37 and 2.49 [IU/dL]/[IU/kg], respectively) values were used from the PK crossover study (Konkle, et al. Blood 2015) of antihemophilic factor (recombinant) (ADVATE®, Shire, Lexington, MA, USA) and rurioctocog alfa pegol (SHP660, BAX 855, ADYNOVATE®, Shire). The model included 3 prophylaxis regimens: SHL-rFVIII 30 IU/kg every other day (EOD), SHL-rFVIII 35 IU/kg 3x/week, and EHL-rFVIII 45 IU/kg 2x/week, as well as a range of theoretical baseline FVIII activity levels with minimal variance (5%, 10%, 15%, and 20%). Hypothetical activity profiles were created using the activity categories from the National Hemophilia Foundation "Playing It Safe - Bleeding Disorders, Sports and Exercise" report (Anderson & Forsyth, 2017), where Type 1, 2, and 3 activities represent low risk of collisions, collisions might occur, and collisions will occur, respectively. The 6 profiles modeled were: Profile 1, Mon through Fri (M-F) Type 1 activity, Sat through Sun (Sat-Sun) Type 3; Profile 2, M-F Type 2, Sat-Sun Type 1; Profile 3, Mon through Sun (M-Sun) Type 2; Profile 4, M-F Type 3, Sat-Sun Type 1; Profile 5, M-F Type 1, Sat-Sun Type 2; and Profile 6, M-F no activity, Sat-Sun Type 1. Bleeding risk by activity category and FVIII level at the time of activity was estimated using odds ratios from Broderick et al. (JAMA 2012). For each regimen, the infusion schedule with the lowest bleeding risk for the activity profile was used. The model assumed each activity occurred 30 min after infusion time for SHL-rFVIII or EHL-rFVIII, but not for baseline FVIII scenarios. Relative bleeding risks were compared between regimens.
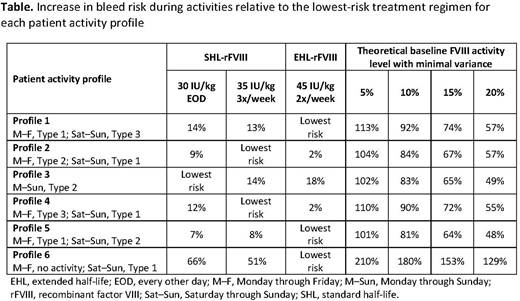
Results: Patients with activity Profile 1, 5, and 6 would be best protected with EHL-rFVIII 2x/week, those with activity Profile 2 and 4 would be best protected with SHL-rFVIII 3x/week, and those with activity Profile 3 would be best protected with SHL-rFVIII EOD (Table). Although some regimens were associated with an only slightly higher risk (2-9%) of bleeding, others imposed a moderately increased risk (12-66%), and baseline FVIII activity levels conferred a higher bleed risk (48-210%) in each of the 6 activity profile types, compared with the most protective regimen.
Conclusion: Considering estimated bleeding risks and predicted FVIII levels for different patient physical activity profiles, this model suggests that tailored dosing regimens with SHL-rFVIII or EHL-rFVIIII can offer a reduced relative bleeding risk during activities versus a baseline FVIII activity level with minimal variance. This highlights the importance of FVIII peaks to ensure optimal protection levels during activity. Personalized treatment using different products and regimens that take into account the patient's level of physical activity may help to optimize protection from bleeding. Further study of bleed-event rates during different physical activities would be of value for the hemophilia community.
Watt:Shire: Employment, Equity Ownership. Epstein:Stratevi: Employment, Equity Ownership. Xuan:Stratevi: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal